
 By Atlantic Endo Medical Review Board
By Atlantic Endo Medical Review Board
More than 40% of American adults are currently classified as obese by traditional BMI standards, yet emerging research suggests that number could be closer to 70% or even higher when more precise body fat measurements are factored in. That gap tells an important story about what BMI can and cannot do for your health.
This Ultimate Guide to Body Mass Index (BMI): Comprehensive Analysis is designed to give you a thorough, clinically grounded comprehension of BMI, how it is calculated, what it means, where it falls short, and how modern medicine is moving beyond it to deliver more accurate health assessments. Whether you are managing a chronic condition, working toward a healthier weight, or simply trying to understand your lab results, this guide will help you make sense of the numbers.
Weight Loss Clinic in Queens, NY.
Table of Contents
Key Takeaways
- BMI is a useful screening tool, but it does not distinguish between fat, muscle, and bone mass.
- Weight category alone does not determine health risk, fat distribution, metabolic markers, and lifestyle factors all matter.
- New research shows that waist-to-height and waist-to-hip ratios significantly improve obesity detection beyond BMI alone.
- A normal BMI does not guarantee good metabolic health; some individuals with normal BMI still carry dangerous levels of abdominal fat.
- Comprehensive body composition analysis, combined with clinical evaluation, provides a far more complete health picture than BMI alone.
What Is BMI and How Is It Calculated?
Body Mass Index is a numerical value derived from a person’s height and weight. The formula is straightforward:
BMI = weight (kg) / height (m²)
For those using imperial measurements, the formula becomes:
BMI = [weight (lbs) / height (in²)] x 703
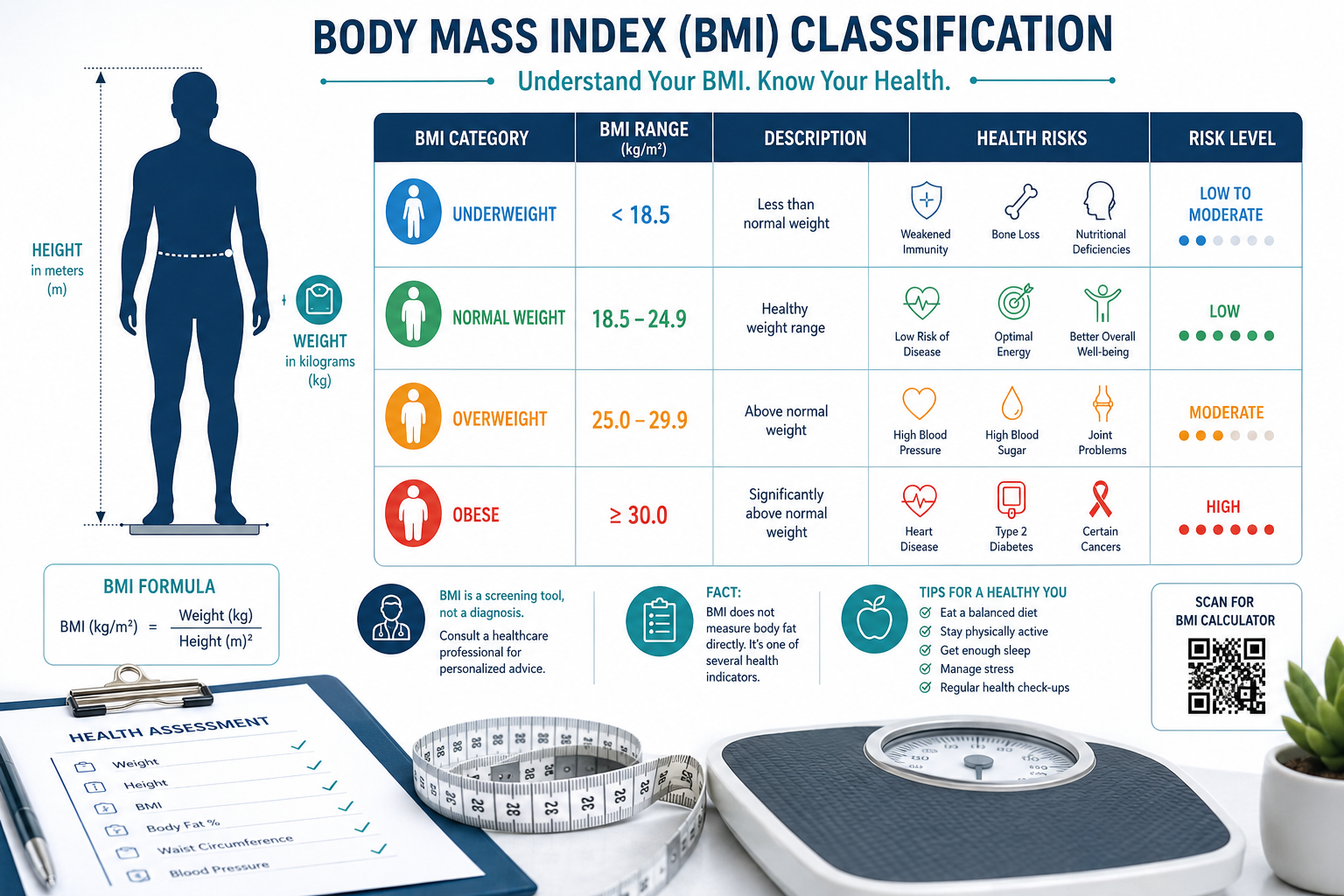
The result places you into one of four standard categories established by the World Health Organization and the Centers for Disease Control and Prevention (CDC):
| BMI Range | Weight Category | General Health Implication |
|---|---|---|
| Below 18.5 | Underweight | Possible nutrient deficiency, bone loss risk |
| 18.5-24.9 | Normal weight | Generally associated with lower chronic disease risk |
| 25.0-29.9 | Overweight | Elevated risk for cardiovascular and metabolic conditions |
| 30.0 and above | Obese | Significantly higher risk for diabetes, heart disease, joint problems |
BMI was originally developed in the 1830s by Belgian mathematician Adolphe Quetelet as a population-level statistical tool, not as an individual clinical diagnostic. It was later adopted by the medical community as a convenient, low-cost screening measure because it requires nothing more than a scale and a measuring tape.
Why BMI Became the Standard
Its appeal is practical: it is fast, inexpensive, and reproducible. Clinicians can calculate it in seconds, and it correlates reasonably well with body fat levels at the population level. For large-scale public health tracking, BMI remains a valuable benchmark.
Nevertheless, that convenience comes with significant trade-offs when applied to individual patients, a limitation that modern endocrinology is actively working to address.
The Critical Limitations of BMI in Clinical Practice

Compehending the limits of BMI is just as important as knowing the formula. This comprehensive analysis of Body Mass Index reveals several well-documented shortcomings that every patient should be aware of.
BMI Does Not Measure Body Composition
BMI cannot distinguish between fat mass, muscle mass, and bone density. A highly trained athlete with substantial muscle may register as “overweight” or even “obese” on the BMI scale, while a sedentary individual with low muscle and high body fat may appear in the “normal” range. This is sometimes called the “normal-weight obesity” phenomenon.
Research confirms this concern: over 25% of U.S. adults with a normal BMI meet clinical criteria for obesity when abdominal fat and weight-related health conditions are factored in. In other words, a reassuring BMI number can mask serious metabolic risk.
Clinical insight
One in four people with a “normal” BMI may carry dangerous levels of visceral fat, the type stored around internal organs, which significantly raises the risk for type 2 diabetes, cardiovascular disease, and hormonal imbalances.
This is why body composition analysis has become an essential complement to BMI in modern clinical practice. Knowing what your body is actually made of, not just how much it weighs, is far more clinically meaningful.
BMI Varies by Age, Sex, and Ethnicity
BMI thresholds were largely developed using data from white European populations. Research consistently shows that individuals of Asian descent carry higher metabolic risk at lower BMI values, while some African American populations may have different body fat distributions that affect risk interpretation. Age also matters: older adults often lose muscle mass while gaining fat, meaning their BMI can remain stable even as their metabolic risk increases.
Fat Distribution Matters More Than Total Weight
Where fat is stored in the body has a profound impact on health outcomes. Visceral fat, concentrated around the abdomen and internal organs, is metabolically active and inflammatory. Subcutaneous fat, stored just beneath the skin, carries lower risk.
This is why measures such as waist circumference, waist-to-height ratio, and waist-to-hip ratio are increasingly recognized as stronger predictors of metabolic disease than BMI alone. When these measurements are incorporated into obesity assessments, the estimated prevalence of obesity among U.S. adults rises to approximately 75%, a dramatic shift from the 40% figure produced by BMI alone.
For patients managing conditions such as type 2 diabetes, PCOS, or thyroid disease, comprehending fat distribution is especially critical. Learning about what body composition actually measures can help you ask better questions at your next appointment.
The Lancet Commission’s Updated Framework
In early 2025, the Lancet Diabetes and Endocrinology Commission released an updated obesity framework that incorporates body fat distribution measures alongside BMI. Applying this framework to over 300,000 individuals revealed that obesity prevalence jumps from roughly 40% to 70%, with the most pronounced effect in older adults. This landmark shift in clinical thinking reinforces that BMI alone is no longer sufficient for comprehensive obesity assessment.
Beyond BMI: Modern Tools for Comprehensive Health Assessment
Given BMI’s limitations, what should patients and clinicians use instead? The answer is not to abandon BMI but to use it as one data point within a broader, more complete evaluation.
Body Composition Analysis
Body composition analysis measures the actual percentages of fat, muscle, water, and bone in your body. Technologies such as bioelectrical impedance analysis (BIA) and DEXA scanning provide far more clinically useful data than a simple height-to-weight ratio. At Atlantic Endocrinology, our body composition analysis services in New York are designed to give patients and their care teams a precise, actionable picture of health.
Resting Metabolic Rate Testing
Your resting metabolic rate (RMR) tells you how many calories your body burns at rest, a critical number for designing effective weight management strategies. Two people with identical BMIs can have vastly different metabolic rates, meaning a one-size-fits-all diet plan will not work for both. Knowing your metabolism and basal metabolic rate helps personalize nutrition and treatment plans.
Waist Measurements and Cardiovascular Risk
Waist circumference is a simple, low-cost measurement that adds significant clinical value. General guidelines suggest that waist circumference above 35 inches in women and above 40 inches in men indicates elevated cardiovascular and metabolic risk, regardless of BMI category. Pairing this with understanding how being overweight affects joints and muscles provides a fuller picture of how excess fat affects daily function.
Hormonal and Metabolic Lab Work
For patients with endocrine conditions, weight and fat distribution are deeply connected to hormone levels. Thyroid dysfunction, insulin resistance, cortisol imbalances, and PCOS can all affect how and where the body stores fat. A comprehensive evaluation by an endocrinologist goes far beyond BMI to assess fasting glucose, insulin levels, lipid panels, thyroid function, and other main markers. Learning how to balance hormones for weight loss is often a critical piece of the puzzle for patients who struggle despite healthy lifestyle efforts.
Emerging Technology: Smartphone-Based Assessment
Recent research has introduced smartphone-based body composition tools that use photographic imaging and deep learning algorithms to estimate body fat percentage and distribution. These technologies are showing promising accuracy and may soon offer scalable, accessible screening options, though they remain supplementary to clinical evaluation at this stage.
BMI in the Context of Chronic Disease Management
For patients already managing chronic conditions, BMI is a starting point, not a destination. Here is how it intersects with common endocrine and metabolic conditions:
- Type 2 Diabetes: Excess visceral fat drives insulin resistance. Even modest reductions in body fat, not just weight, can dramatically improve blood sugar control.
- Thyroid Disease: Hypothyroidism can cause weight gain that inflates BMI, while hyperthyroidism can cause unintended weight loss. Neither scenario is accurately captured by BMI alone.
- PCOS: Women with polycystic ovarian syndrome often struggle with weight gain driven by insulin resistance and hormonal imbalance, making body composition analysis especially valuable.
- Cardiovascular Disease: Abdominal obesity is a stronger predictor of heart disease risk than overall BMI. Patients with hypertension benefit from a full metabolic and body composition workup.
- Bone Health: Both underweight and obese individuals face elevated bone disease risk, though for different reasons. Preventing bone disease requires comprehending the relationship between body composition and bone density.
How Atlantic Endocrinology Approaches Weight and Body Composition
At Atlantic Endocrinology & Diabetes Center, we take a multidisciplinary, patient-centered approach to weight and metabolic health. Our team, led by Dr. Stella Ilyayeva, M.D., an endocrinology specialist with over 20 years of experience, understands that BMI is just one piece of a complex clinical picture.
We offer:
- Body Composition Analysis at our Queens and Brooklyn locations
- Resting Metabolic Rate Testing to personalize nutrition and weight plans
- Comprehensive laboratory services including hormonal panels, lipid profiles, and metabolic markers
- Semaglutide injections and medical weight management for eligible patients
- Nutrition and wellness counseling integrated with endocrine care
- Cardiology, podiatry, and physical therapy for patients with weight-related complications
Our comprehensive weight management program is designed to treat the whole patient, not just a number on a scale.
We accept most major insurance plans including Aetna, United Healthcare, Medicaid, Medicare, Healthfirst, EmblemHealth, and many others. Our four convenient locations in Queens and Brooklyn are here to serve you.
FAQs
Is BMI an accurate measure of health for everyone?
BMI is a useful population-level screening tool, but it has well-documented limitations for individuals. It does not account for muscle mass, bone density, age, sex, or ethnicity. A person with high muscle mass may register as overweight despite excellent metabolic health, while someone with normal BMI may carry dangerous levels of visceral fat. Clinicians are increasingly using BMI alongside waist measurements, body composition analysis, and laboratory work for a more complete assessment.
What BMI is considered healthy for adults?
The CDC and WHO define a BMI between 18.5 and 24.9 as “normal weight” for most adults. Nonetheless, healthy BMI ranges can vary by age and ethnicity. For example, many clinical guidelines recommend lower BMI thresholds for individuals of Asian descent, where metabolic risk increases at BMIs above 23. Always discuss your individual BMI target with your healthcare provider in the context of your full health profile.
Can I have a normal BMI and still be at risk for metabolic disease?
Yes. Research shows that more than 25% of adults with a normal BMI meet clinical criteria for obesity when abdominal fat and metabolic health markers are evaluated. This condition, sometimes called “normal-weight obesity” or “metabolically obese normal weight,” is associated with elevated risk for type 2 diabetes, cardiovascular disease, and other chronic conditions. This is one of the strongest arguments for going beyond BMI in clinical assessments.
How often should I have my BMI and body composition checked?
For most adults, annual screening is a reasonable baseline. Nevertheless, individuals managing chronic conditions such as diabetes, thyroid disease, PCOS, or cardiovascular disease may benefit from more frequent monitoring. Your endocrinologist or primary care provider can recommend a schedule based on your specific health goals and risk factors. If you have concerns about your weight or body composition, scheduling a comprehensive evaluation is the best first step.
References
- Centers for Disease Control and Prevention. (2022). About Adult BMI. https://www.cdc.gov/bmi/about/index.html
- Deurenberg, P., Yap, M., & van Staveren, W. A. (2021). Body mass index and percent body fat: A meta-analysis among different ethnic groups. International Journal of Obesity, 22(12), 1164-1171. https://doi.org/10.1038/sj.ijo.0800741
- Lancet Diabetes & Endocrinology Commission. (2025). Redefining obesity: A new framework for clinical and public health practice. https://www.thelancet.com/commissions/obesity
- National Institutes of Health, National Heart, Lung, and Blood Institute. (2023). Assessing Your Weight and Health Risk. https://www.nhlbi.nih.gov/health/educational/lose_wt/BMI/bmicalc.htm
- Harvard T.H. Chan School of Public Health. (2022). The Nutrition Source: Obesity prevention source, BMI and waist circumference. https://www.hsph.harvard.edu/obesity-prevention-source/obesity-definition/
Medical and Editorial Commitment
The content of this article is strictly for educational and informational purposes. It does not replace in-person professional medical diagnosis, advice, or treatment..
Read Privacy PolicyRelated Posts

How to Lose 10 kg in 7 Days? Truth Explained — What a Weight Loss Clinic in Queens, NY Really Recommends
Last updated: May 26, 2026 Quick Answer: Losing 10 kg of actual body fat in 7 days is not physiologically possible without [...]

Do B12 Injections Work for Weight Loss and Energy Changes
You’ve heard the buzz about B12 injections for effortless weight loss and a major energy boost. It sounds almost too good to [...]