
 By Atlantic Endo Medical Review Board
By Atlantic Endo Medical Review Board
More than 3 million people in the United States are living with von Willebrand disease (VWD) — yet most have never heard of it. Unlike hemophilia, which receives far more public attention, VWD is actually the most common inherited bleeding disorder in the world, affecting approximately 1% of the general population equally across males and females. If you or someone you love experiences unexplained bruising, prolonged nosebleeds, or unusually heavy menstrual cycles, comprehending this condition could be life-changing.
For patients seeking expert Hematology in Queens, NY, Atlantic Endocrinology & Diabetes Center offers multidisciplinary care that connects you with the right specialists, the right diagnostic tools, and a team that genuinely listens.
Begin Evaluation Hematology in Queens, NY.
Table of Contents
Key Takeaways
- Von Willebrand disease is the most common inherited bleeding disorder, affecting roughly 1 in 100 people worldwide.
- It is caused by a deficiency or dysfunction of von Willebrand factor (VWF), a protein essential for normal blood clotting.
- VWD affects males and females equally, though symptoms are often more noticeable in women due to menstrual bleeding.
- Treatment options have expanded significantly, including a major FDA approval in 2025 for a recombinant VWF therapy now available for both adults and children.
- Early diagnosis and specialized hematological care can dramatically reduce the risk of serious bleeding episodes.
What Is Von Willebrand Disease and Why Does It Matter?
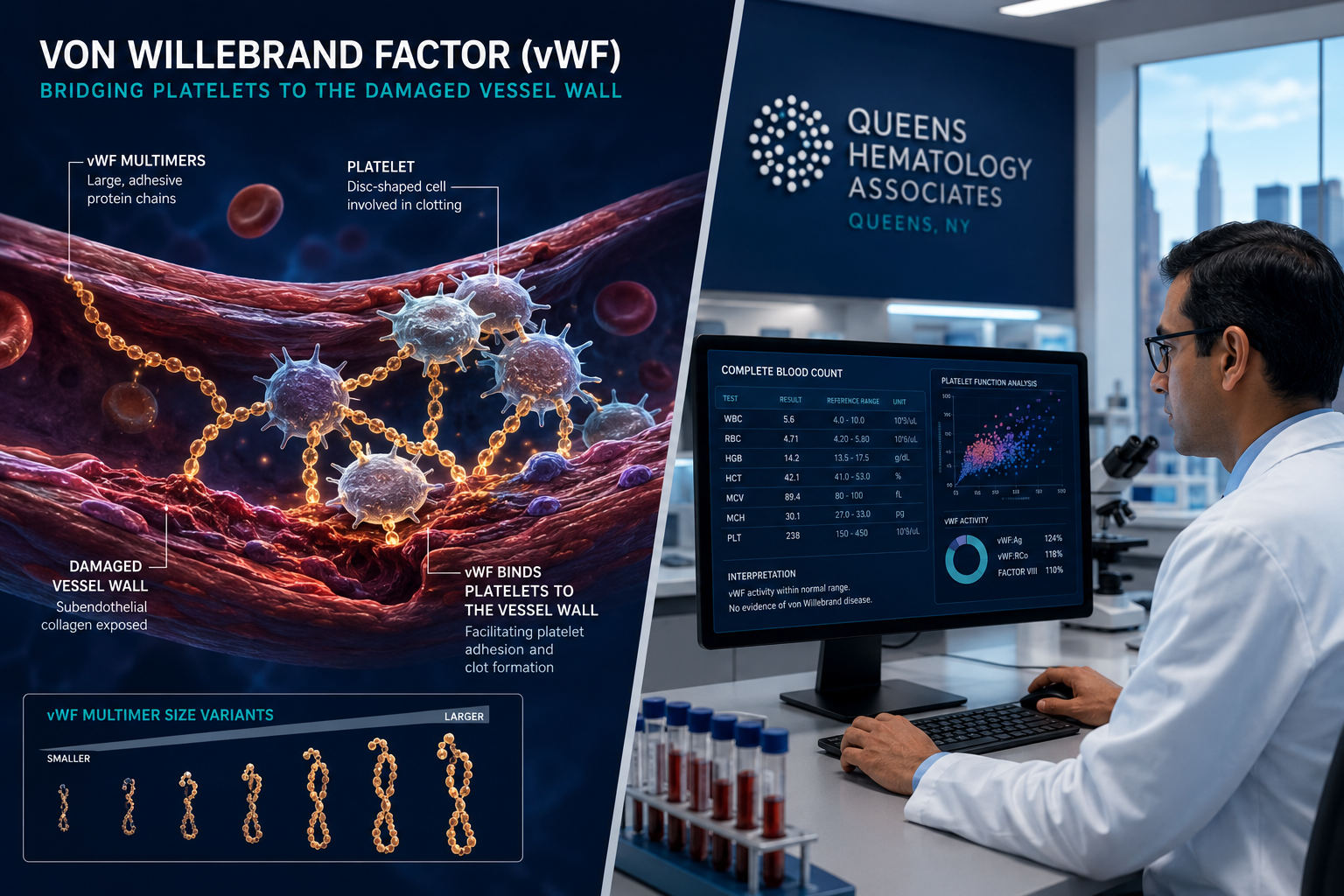
Von Willebrand disease is a hereditary bleeding disorder caused by a deficiency or abnormality in von Willebrand factor (VWF), a large multimeric protein produced in the cells lining blood vessels and in platelets. VWF plays two critical roles: it acts as a bridge that helps platelets stick to damaged vessel walls, and it carries and protects Factor VIII, another clotting protein. When VWF is absent, reduced, or not working properly, the blood cannot form a stable clot efficiently.
There are three main types of VWD:
| Type | Description | Severity |
|---|---|---|
| Type 1 | Partial quantitative deficiency of VWF | Mild to moderate |
| Type 2 | Qualitative defect (VWF present but dysfunctional) | Moderate |
| Type 3 | Near-complete absence of VWF | Severe |
Type 1 is the most common, accounting for the majority of cases. Type 3 is the rarest but most severe form.
Common Symptoms to Watch For
Many people with VWD live for years without a formal diagnosis because their symptoms seem ordinary or unrelated. Main warning signs include:
- Prolonged or heavy nosebleeds lasting more than 10 minutes
- Easy bruising with no clear cause
- Heavy menstrual bleeding (menorrhagia), often misattributed to hormonal issues
- Prolonged bleeding after dental work, surgery, or minor cuts
- Joint or muscle bleeding (more common in severe Type 3)
- Gastrointestinal bleeding in some cases
Because heavy menstrual bleeding is a hallmark symptom, many women with VWD are initially evaluated for hormonal conditions. If you have been exploring what symptoms would prompt a visit to an endocrinologist, it is worth knowing that bleeding disorders and hormonal health can intersect in meaningful ways.
Who Is at Risk
VWD is inherited in an autosomal dominant pattern in most cases, meaning a single copy of the altered gene is enough to cause the condition. If one parent has VWD, each child has a 50% chance of inheriting it. Type 3 VWD follows an autosomal recessive pattern, requiring two defective gene copies.
Because the condition affects males and females equally, it should never be dismissed as “just a female problem” or overlooked in men who report unusual bleeding patterns.
Diagnosing and Treating VWD: Advances in Hematology in Queens, NY

Diagnosing VWD has historically been challenging. Blood levels of VWF naturally fluctuate with stress, exercise, pregnancy, and even blood type — people with Type O blood tend to have lower VWF levels. This variability means that a single normal test result does not rule out the condition.
Newer Diagnostic Tools
Recent advances in laboratory science have produced more precise assays for VWD diagnosis. Two newer tests — VWF:GPIbM and VWF:GPIbNab — offer improved sensitivity over older platelet-binding assays. These tools allow hematologists to classify VWD subtypes with greater accuracy, which directly affects treatment decisions.
A standard diagnostic workup typically includes:
- VWF antigen test — measures the amount of VWF protein in the blood
- VWF activity test (Ristocetin cofactor assay) — measures how well VWF functions
- Factor VIII activity level — since VWF carries Factor VIII
- Complete blood count (CBC) — to assess platelet levels
- Bleeding time or platelet function assay
For patients in New York, access to advanced Queens medical laboratory services can make this diagnostic process smoother and more efficient.
Current Treatment Options
Treatment for VWD depends on the type and severity of the condition, as well as the clinical situation (routine prevention versus acute bleeding).
1. Desmopressin (DDAVP)
This synthetic hormone stimulates the release of stored VWF from blood vessel walls. It is the first-line treatment for most Type 1 VWD patients and works well for mild-to-moderate cases. It can be given intravenously, by injection, or as a nasal spray.
2. VWF Replacement Therapy
For patients who do not respond to desmopressin — including most Type 2 and all Type 3 patients — replacement therapy using plasma-derived or recombinant VWF concentrates is used.
In September 2025, the FDA approved an expanded use of Vonvendi, a recombinant von Willebrand factor product, for routine prophylaxis in adults with all types of VWD and for on-demand treatment in pediatric patients. This marked a significant milestone as the first recombinant VWF product approved for use in children in the United States. The approval was granted under Priority Review and carries Orphan Drug Designation, reflecting the urgency of addressing this underserved condition.
3. Antifibrinolytic Agents
Medications such as tranexamic acid and aminocaproic acid prevent the breakdown of blood clots once they form. They are particularly useful for managing mucosal bleeding, heavy menstrual periods, and bleeding after dental procedures.
4. Hormonal Therapies
For women with VWD, hormonal contraceptives can raise VWF levels and reduce menstrual blood loss. This is one reason why the intersection of hematology and hormonal health is so important — a topic well understood by the multidisciplinary team at Atlantic Endocrinology.
Emerging Therapies on the Horizon
The treatment landscape for VWD is evolving rapidly. In June 2026, Incyte Corporation acquired Vega Therapeutics for $1.25 billion, gaining access to a late-stage drug candidate designed to offer a less burdensome dosing schedule than current therapies. Additionally, research published in April 2026 introduced HMB-002, a monovalent antibody that binds to VWF and extends its half-life while preserving its physiological function. In nonhuman primate studies, it raised VWF and Factor VIII levels by approximately twofold — a promising finding for future clinical development.
These advances reflect what personalized medicine and precision medicine are making possible: treatments tailored not just to the disease, but to the individual patient’s biology.
When to See a Hematologist
Many people delay seeking care because they assume their symptoms are normal. You should consider seeing a hematologist if you experience:
- Unexplained or frequent nosebleeds
- Bleeding that takes unusually long to stop
- Heavy periods that interfere with daily life
- A family history of bleeding disorders
- Abnormal bleeding during or after surgery
Knowing when to see a hematologist and recognizing common warning signs is the first step toward getting the answers you deserve.
The Connection Between VWD and Other Health Conditions
VWD does not exist in isolation. Patients managing chronic conditions — including diabetes, thyroid disease, and cardiovascular issues — may find that their overall health status affects bleeding risk and treatment response. For example, thyroid hormones influence VWF levels; hypothyroidism can lower them, potentially worsening bleeding symptoms. This is precisely why a multidisciplinary approach matters.
At Atlantic Endocrinology & Diabetes Center, hematology care works alongside endocrinology, cardiology, and other specialties. If you are already managing a condition like diabetes and want to know what organ is most affected by glucose, or if you are concerned about how a chronic condition may interact with a bleeding disorder, our team can help you see the full picture.
For patients with blood-related concerns beyond VWD, resources like our guide on treatment for CML chronic myelogenous leukemia demonstrate our commitment to comprehensive hematological education.
Living Well with VWD
A VWD diagnosis does not have to limit your life. With the right care team and treatment plan, most patients manage their condition effectively. Practical strategies include:
- Carrying a medical alert card identifying your diagnosis and treatment plan
- Communicating proactively with all healthcare providers, including dentists and surgeons
- Avoiding NSAIDs (like ibuprofen and aspirin) that impair platelet function
- Maintaining a healthy weight to reduce stress on joints and minimize injury risk
- Monitoring menstrual cycles carefully and reporting changes to your doctor
For women, the hormonal dimension of VWD management makes it especially important to have access to both hematological and endocrinological expertise in one place. If you have questions about how hormonal health intersects with your overall wellness, exploring hormone replacement therapy and weight loss may offer useful context.
Your Path to Expert Hematology in Queens, NY
Atlantic Endocrinology & Diabetes Center serves patients across Queens and Brooklyn with a team of dedicated specialists who understand that complex conditions require coordinated care. Whether you are newly diagnosed, seeking a second opinion, or managing VWD alongside other chronic conditions, we are here to support you.
Our locations:
- Rego Park: 97-25 63 Dr 1 FL, Rego Park, NY 11374 | Mon–Thu: 9 AM–7 PM
- Forest Hills: 99-45 67th Rd Suite 103, Forest Hills, NY 11375 | Mon, Tue, Thu: 9 AM–5 PM
- Bushwick/Brooklyn: 359 Stockholm Street, Brooklyn, NY 11237 | Mon: 9 AM–7 PM
- Better Health Clinic: 97-32 63rd Rd, Rego Park, NY 11374 | Mon–Thu: 9 AM–7 PM
We accept most major insurance plans including Aetna, Cigna, Medicaid, Medicare, United Healthcare, EmblemHealth, Healthfirst, Fidelis Care, and many others.
To schedule an appointment, visit atlanticendomd.com/contact or call (718) 275-2900.
FAQs:
Is von Willebrand disease curable?
VWD is a lifelong genetic condition and is not currently curable. Nevertheless, it is highly manageable. Most patients with Type 1 VWD lead normal, active lives with minimal intervention. More severe forms require ongoing treatment, but advances in recombinant VWF therapy and emerging biologics are making long-term management safer and more convenient than ever before.
Can VWD be mistaken for another condition?
Yes, frequently. Women with VWD are often told their heavy periods are hormonal in origin. Others are diagnosed with iron-deficiency anemia without identifying the underlying bleeding disorder as the cause. Because VWF levels fluctuate naturally, a single normal lab result can be misleading. Repeated testing and newer diagnostic assays like VWF:GPIbM offer more reliable results. If you have persistent bleeding symptoms, ask specifically about VWD testing.
Does VWD affect children differently than adults?
Children with VWD may present with nosebleeds, easy bruising, or prolonged bleeding after minor injuries. The September 2025 FDA approval of Vonvendi for pediatric on-demand use was a major step forward, as it provided the first recombinant VWF option for children in the U.S. Early diagnosis in children allows families and school staff to prepare appropriately and reduces the risk of serious bleeding events during activities.
How is VWD different from hemophilia?
Both are inherited bleeding disorders, but they differ in mechanism and demographics. Hemophilia A and B are caused by deficiencies in Factor VIII and Factor IX, respectively, and primarily affect males. VWD affects both sexes equally and involves a deficiency or dysfunction of von Willebrand factor, which also carries Factor VIII. VWD is far more common than hemophilia, though it is generally less severe in most patients.
References
Centers for Disease Control and Prevention. (2024). Von Willebrand Disease (VWD). https://www.cdc.gov/bleeding-disorders/about/vwd.html
National Hemophilia Foundation. (2023). Von Willebrand Disease. https://www.hemophilia.org/bleeding-disorders-a-z/types/von-willebrand-disease
U.S. Food and Drug Administration. (2025). FDA Approves Expanded Use of Vonvendi (von Willebrand factor recombinant). https://www.fda.gov/news-events/press-announcements/fda-approves-expanded-use-vonvendi-von-willebrand-disease-including-certain-uses-children
Leebeek, F. W. G., & Eikenboom, J. C. J. (2021). Von Willebrand’s Disease. New England Journal of Medicine, 375(21), 2067–2080. https://www.nejm.org/doi/full/10.1056/NEJMra1601561
National Organization for Rare Disorders (NORD). (2022). Von Willebrand Disease. https://rarediseases.org/rare-diseases/von-willebrand-disease/
Medical and Editorial Commitment
The content of this article is strictly for educational and informational purposes. It does not replace in-person professional medical diagnosis, advice, or treatment..
Read Privacy PolicyRelated Posts

How a Neurologist in Queens, NY Can Help Treat Neurological Sleep Disorders in Older Adults
Nearly 50% of adults over the age of 65 report chronic sleep problems — yet fewer than 15% ever receive a formal [...]

How It Works in the Rehabilitation of Amputees in Queens, NY
Connect With Experts Physical Therapy in Queens, NY. More than 185,000 amputations are performed in the United States every year, and diabetes [...]